Prophylaxis
Prophylaxis (from the Greek phylassein, "be vigilant") is a collective term for all measures taken to prevent from the outset any impairments to health, their persistence, increase or reoccurrence. Chronologically, therefore, it mainly occurs prior to examinations for screening or early detection and minimally invasive treatment. Nowadays the modern terms prophylaxis and prevention are often used synonymously.
Prophylactic measures are classified according to various criteria:
Target group: They can be targeted at individual persons (individual prophylaxis), a specific population (group prophylaxis) or the entire population (collective prophylaxis). They are differentiated according to age group as infant-, child-, adolescent-, adult- and geno-prophylaxis and also according to the current physical status as pregnancy prophylaxis or handicapped prophylaxis.
Methods: Different types of methods can be used for prophylaxis, e.g. clarification about and application of behaviour patterns, mechanical and technical aids, preventive use of pharmacological and chemical active agents or vaccines.
Performed by: Measures can be performed by the person affected (oral self-care) or by other persons, mainly medical specialists (professional oral-care).
Disease pattern: Prophylaxis, which is completed on healthy patients (primary prophylaxis), should be differentiated from early detection of incipient disease processes (screening, secondary prophylaxis) and the prevention of relapses after completed treatment (tertiary prophylaxis). Primary-primary prophylaxis is used for pregnant women and is aimed at the unborn child.
Dental prophylaxis is mainly targeted towards caries prevention and periodontitis prophylaxis. One of the central objectives of dental prophylaxis is clarification about and implementation of measures for the control and regular removal of dental plaque (plaque control). It is mainly completed via domestic oral hygiene using aids for mechanical cleaning of occlusal, oral and buccal tooth surfaces (manual and electric toothbrushes, toothpastes), the interdental spaces (dental floss, interdental brushes, toothpicks). Bacterial reduction using disinfectant mouthwash (e.g. with chlorhexidine) can also be a sensible measure (chemoprophylaxis). The dentist can support prophylactic treatment by performing professional tooth cleaning.
Cleaning the tongue (tongue scraper) achieves halitosis prophylaxis.
Periodontal prophylactic measures include restricting or giving up the consumption of tobacco products, correct cessation of manifest diabetes and gingivitis prophylaxis.
Restriction or avoidance of drinks (soft drinks) or food (honey, sweets) with a high sugar content is an effective method of caries prevention. Sealing of caries-free fissures and pits by the dentist is also effective. Fluorides are also used for this purpose, e.g. collective prophylactic fluoridation of drinking water and salt, group and individual prophylactic measures using the application of fluoride gels and varnishes as well as by the use of fluoride toothpastes.
In the case of patients with serious pre-existing diseases or heart abnormalities, administration of antibiotics for endocarditis prophylaxis is required prior to invasive dental procedures.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| polishing debris | Polierreste |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms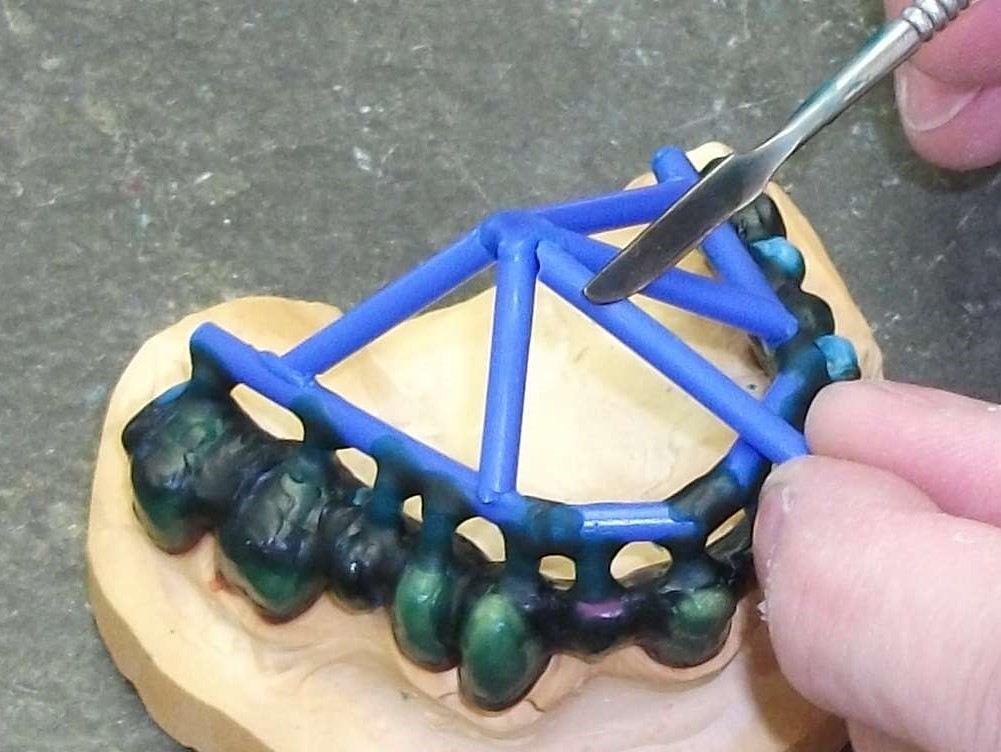 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument