Wax build-up technique
Wax build-up technique
The term wax build-up technique describes dental technical procedures for waxing up the exterior contours of crowns and bridge units when fabricating prosthetic restorations in the laboratory. Functionally correct design of the occlusal surfaces of the posterior teeth is particularly important for cast restorations. Depending on the school of thought (e.g. P.K. Thomas, Lundeen/Payne, Polz, Schulz), various tooth-to-tooth relationships, occlusal concepts, cusp-to-fossa relationships and contact area patterns are preferred.
The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes).
The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers.
Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
 Wax preforms
Wax preforms
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
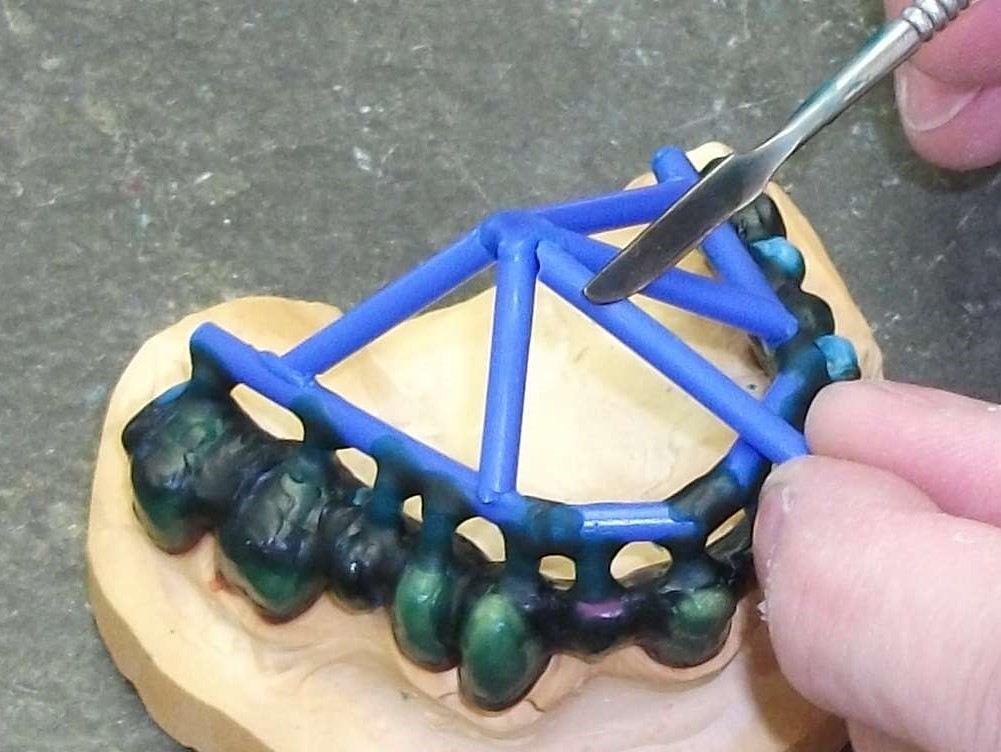 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed.
Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| fluorosis marking | Fluorosefleck |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration