Periodontology
Periodontology is that branch of dentistry involved with the healthy and sick periodontium ("attachment apparatus"), i.e. those anatomical structures surrounding, supporting and retaining the tooth. These include the marginal periodontium or gingiva (free marginal and attached gingiva), desmodontium (connective tissue in the periodontal cleft with hemi-desmosomes, Sharpey's fibres, cementum) and bony socket (alveolar bone).
A healthy periodontium is considered a prerequisite for every other type of dental treatment, in particular prosthodontics and implants. Many aspects of periodontology also apply to implant treatment – this is referred to as peri-implantology.
Periodontal diseases
The estimated prevalence is 75%. Chronic or acute forms of these diseases can be divided into degrees of severity (superficial, profund, aggressive), the age of onset (juvenile, adult), spread (local, general) or the cause. The different inflammatory forms ("periodontitis" - lay term: "periodontosis", and "peri-implantitis" involving implants) are virtually always due to bacteria. Hereditary factors (e.g. immune system), the anatomical situation (ligament attachments, malocclusion), functional overloading (bruxism), behavioural aspects (e.g. oral care, nutrition, smoking), medicines (anti-epileptic, anti-hypertensive medication, chemotherapy), hormone balance (menstruation, pregnancy, hormone substitution) and systemic diseases (metabolic or immunological diseases, tumours) also play a role. Periodontitides and diabetes have been proven to promote the effects mutually.
Periodontitis is often a result of gingivitis along with (due to accumulation of calculus, plaque, bacteria, toxic substances and inflammation mediators) detachment and resorption of the periodontium (formation of deeper gingival pockets) and gingival recession accompanied by loss of bone around the tooth root (intrabony pockets, vertical bone resorption) or even sinking of the entire bony jaw (horizontal bone loss). The visible and perceptible, yet rarely painful, consequences are exposed ("longer") tooth cervixes, mobile, tilting or drifting teeth and even tooth loss.
 Intrabony pockets resulting from periodontitis
Intrabony pockets resulting from periodontitis
When allowed to go untreated, periodontal disease progresses slowly over years or even decades but may worsen intermittently at any time. It usually results in premature loss of some, many or all teeth.
Pulp and periodontium
An apical lesion with endodontic causes is referred to as "apical periodontitis". As the pulp and periodontal cleft communicate with each other anatomically, infections can be transferred from one to the other. This results in "combined lesions" which are complicated to treat.
Screening
Indexes including the pocket probing depth (PPD) and other parameters such as the tendency to bleed (BOP), e.g. the PSI (periodontal screening index) are used for exploratory examination and determination of the necessity for further diagnostics.
Periodontal status
Prior to commencing periodontal treatment the periodontal status must be determined and documented either by hand or electronically. This involves precise measurement of the gingival pocket depths at 2 to 6 defined locations per periodontium as well as further parameters (furcation involvement, recession, tooth mobility and drifting etc.). In addition, an X-ray is taken of all teeth and usually consists of 10 – 14 overlapping individual images ("radiographic status") or a panographic radiograph.
Periodontal treatment
The primary objective of periodontal therapy is to impede or prevent recession of periodontal structures, augment lost sections where necessary, as well as create and maintain easily cared for conditions.
Periodontal pre-treatment involves removing all plaque and calculus (from teeth, gingiva, interdental spaces, restorations) and instructing the patient in the oral care procedures required for the prevention of further plaque accumulation and elimination of risk factors.
The actual periodontal treatment comprises removal of subgingival accretion, inflamed tissue, calculus and infected cementum ("scaling") as well as planing those root surfaces accessible immediately or following surgical exposure (e.g. raising a flap) using hand or ultrasonic instruments (curettes or scalers) to allow reattachment of tissue on the tooth surface.
Periodontal surgical procedures and suturing techniques are employed for contouring the periodontium and/or eliminating deep gingival and bony pockets either partly or in full. In addition, disinfection may be achieved by means of laser (if necessary including the photodynamic therapy yet to be evidence-based), locally active solutions or gels (such as chlorhexidine) as well as local or systemic antibiosis (if necessary following germ determination, such as with DNA probes, for clinical monitoring).
Autogenous or heterogenous tissue (graft) and/or augmentation materials (such as for bone) can be used for augmenting lost anatomical structures. Membranes or blood constituents (such as growth factors) promote and guide regeneration of autogenous periodontal tissue (guided tissue regeneration/GTR, guided bone regeneration/GBR).
Supportive therapy
Once treatment has been completed, the patient attends recall appointments for supportive periodontal therapy (SPT), where possible for the rest of his/her life (such as a regular screening index/scaling and polishing) in order to check and maintain the stable condition already achieved as well as identify and treat relapses at an early stage.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| study period | Versuchsdauer, Versuchszeitraum |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms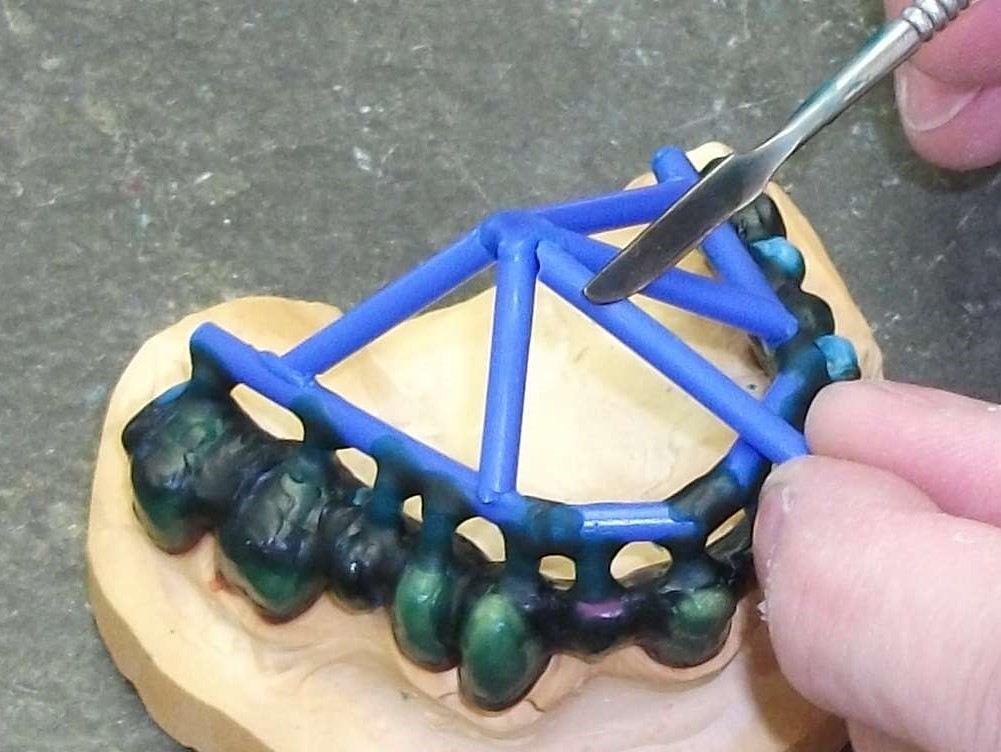 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument