Membranes
Membranes have been used in dental medicine since about 1980 for covering naturally existing, pathologically caused or synthetically created areas of tissue. They function as a barrier. They are intended forpreventing the growth of unwanted tissue into the boundary area as well as shielding and promoting the formation of tissue required within the area using GTR/GBR. The ideal membrane should have the following characteristics: not trigger immune response, non-toxic (biocompatibility), no risk of infection, formable, adaptable and trimmable, adequately firm/rigid and positionally stable, if necessary permeable for substances yet impermeable to cells, time-determinable spacer function, predictable biological degeneration where required.
Non-resorbable membranes
Non-resorbable membranes can, for example consist of cellulose ester, PTFE or titanium. A second surgical intervention is always required to remove them.
Cellulose ester membranes
The first generation of membranes used (approx. 1980) for shielding against bacteria.
PTFE membranes
Flexible, tear-resistant membranes made from ePTFE (expanded polytetrafluorethylene =Teflon®) with micropores, which make exposure a low risk as no cells or microorganisms can pass through. Sometimes they are reinforced with titanium mesh, making them firm and dimensionally stable; highly suitable for covering extensive augmented areas.
Titanium membranes
These approx. 30 µm thick titanium foils are highly suitable for GBR and alveolar ridge augmentation. They are completely impervious and can be prestressed.
Resorbable membranes
No second intervention is required for removing resorbable membranes due to their integration in the tissue. They are the preferred choice where anticipated that permanent full coverage of the membrane by tissue will be possible and tissue support is not the main priority.
The only resorbable membranes used in the dental sector consist of alloplastic materials. In dentistry we differentiate between hydrophobic, synthetic polymer membranes (e.g. made from polylactide) and hydrophilic, xenogeneic (e.g. bovine or porcine) collagen membranes.
Polylactide membranes
These mostly multi-layer membranes are initially rigid but formable intraorally and mainly used for GTR in periodontology and less commonly for GBR. They comprise polymers of the two enantiomers (D and L form) of lactic acids, if necessary supplemented by portions of glycolide. After a 20-week period in situ these membranes begin to degrade hydrolytically over intermediate stages into the end products water and CO2. This process is complete after approx. one year.
Collagen membranes
These membranes are of animal origin (mostly cattle or pigs) and require careful pretreatment in order to prevent the transfer of pathogens. The collagen structure is differentiated between more rigid (synthetic), cross-linked materials and more flexible (native, natural), non-cross-linked materials. Indications for collagens are stabilising extraction alveoli, coverage of bone defects and augmentation materials, prerestorative alveolar ridge augmentation and periodontal surgery.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms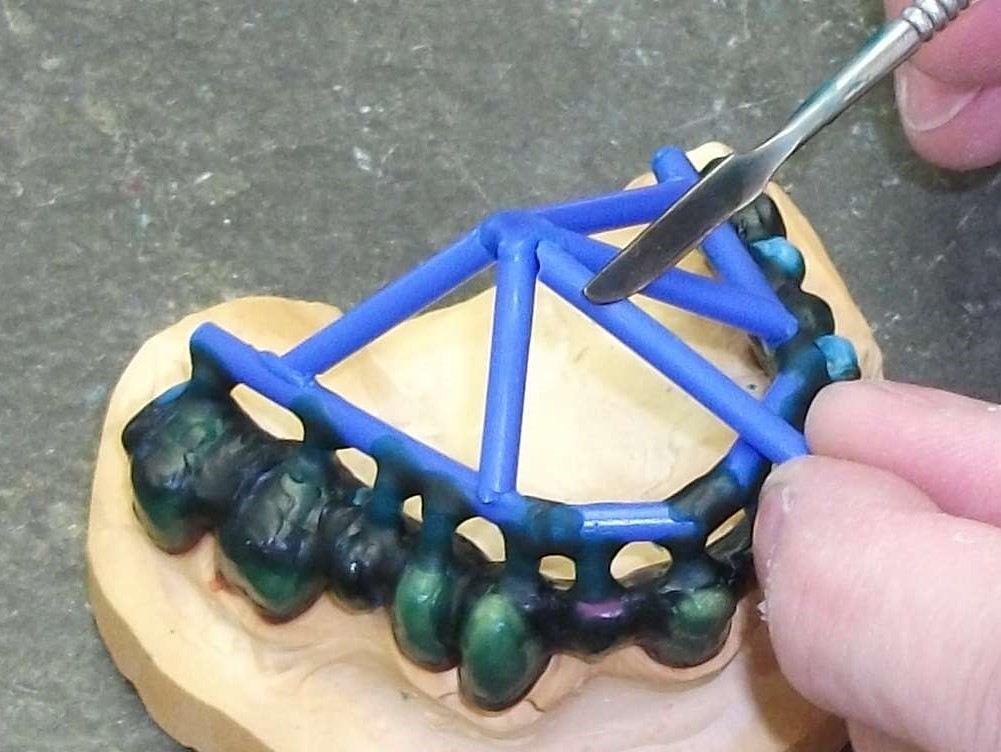 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument