Removable restorations
Removable restorations are a subcategory of prosthetics. Various versions of partial restorations supplement existing teeth and/or implants. Full restorations (full/complete dentures) replace all the teeth in an edentulous jaw (the only prosthetic alternative not involving implants).
A differentiation is made between less expensive, purely removable restorations (this includes full dentures and clasped dentures retained on natural teeth) and more expensive fixed-removable dentures. With more expensive restorations the removable section is anchored using retentive and connector elements (possible options are clasps, attachments, telescope crowns, press-stud systems, magnets etc.) on the periodontally-borne, fixed section of the restoration (mainly in the form of crowns or bridges on teeth and implants).
.jpg) Telescopic denture (wax try-in, stone model)
Telescopic denture (wax try-in, stone model)
 Upper and lower acrylic dentures
Upper and lower acrylic dentures
An overdenture completely covers all connectors and corresponds to a full denture.
Generally, removable restorations cover segments which are extended to a greater or lesser extent, supported by and cover the load-bearing mucosa. During fabrication, the aim is to achieve uniform fit of the removable restoration base on the jaw using special impression materials and procedures. If the resilience of the mucosa is exceeded or if the removable restoration is subjected to repeated rubbing movements, pressure spots may quickly occur. After months and years the bony denture-bearing area resorbs individually by varying degrees (physiological and pressure atrophy). Congruency can be restored by relining the denture base.
The area of the removable restoration that covers the hard palate in the upper jaw is referred to as the palatal plate (fabricated from acrylic or metal) and a section on the edentulous alveolar ridge is referred to as the saddle. Removable restoration saddles are often connected by a metal base (frequently fabricated using CrCo), in the upper jaw possibly using a large connector (transverse connector) and in the lower jaw using a lingual bar. Removable restorations can, however, also be fabricated completely without metal.
 Clasped CoCr denture on stone model
Clasped CoCr denture on stone model
Missing teeth are mostly replaced on saddles by prefabricated denture teeth made from acrylic, less commonly (historically more frequently) also by prefabricated porcelain teeth. In contrast, removable bridges (mainly supported by telescope crowns) replace teeth with solid or veneered pontics and function entirely or as far as possible without mucosal coverage.
Restorations, which are fixed for the patient (possibly screw-retained or semi-permanently cemented), but are designed to be removable by the dentist, are called "operator-removable".
Removable restorations - unlike fixed restorations - allow extraoral care and repair measures. Control and hygiene of the residual teeth are also facilitated. In many cases removable restorations can be extended if load-bearing abutment teeth are lost and a remake is often unnecessary.
With removable restorations placing implants to increase the number of abutments can contribute to firmer, more stable retention and easing of the stress on residual natural teeth.
If a removable restoration is only to be worn temporarily, e.g. for testing a new occlusal relationship or bridging the period required for fabrication of the definitive restoration or other treatment, it is called a temporary restoration. This often involves a simple acrylic denture, with bent wire clasps if necessary. Removable restorations, fitted immediately following surgery (implant placement or extraction), are called immediate restorations.
If other anatomical structures are also replaced by removable restorations in addition to missing teeth, these are referred to as maxillofacial appliance.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| polishing debris | Polierreste |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms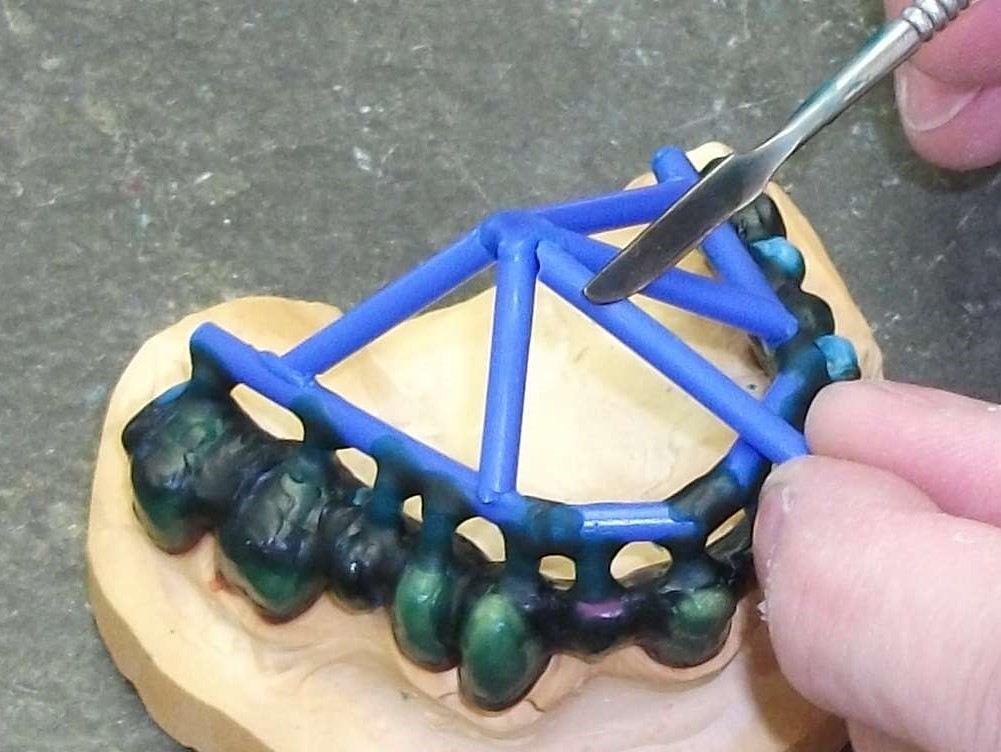 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument