Intraoral scanners
Intraoral scanners
An intraoral scanner is an electronic device for taking so-called digital scans (impressions) of intraoral structures by means of contactless scanning with light rays (visible light/laser) chairside and within seconds or minutes. These devices comprise (as of 2016) a wired handpiece, for intraoral use by the dentist, connected to a computer system with monitor. A combination of a special camera unit in a known three-dimensional position to a light source uses triangulation to calculate the three-dimensional arrangement of the light reflecting surface points of the scanned structures with an accuracy of 20 µm. Each measuring field is usually only about two square centimetres in size but many images (20 to 60 mostly colour video/series images per second) can be taken and merged in quick succession.
To achieve an accurate intraoral scan, (as with every conventional impression) undercuts (possibly non-detectable optically) must be avoided, other obscured (by retraction pastes and cords) areas such as subgingival regions exposed in advance and bleeding staunched. To date, intraoral scanners cannot capture mucosal resilience (important for designing denture bases).
Some systems require additional preparation by coating the imaging area with a thin layer of powder. Implant platforms and their connector geometry are scanned indirectly by placing “scanbodies” i.e., standardised components of known dimensions and clearly aligned three-dimensionally via standardised recesses, on their top surfaces.
When preparing teeth, in real-time parameters such as amount of reduction in tooth structure, distance from opposing dentition, path of insertion and parallelisation of abutment teeth, surface morphology or contours of the preparation margin may be blown-up as required for evaluation and adjustment if necessary. In addition to teeth and/or implants for replacement or treatment, adjacent and opposing teeth as well as the bite may be scanned.
Full digital scans of a jaw may be captured in one procedure or merged one-by-one from overlapping partial images. Specific regions are easily cut out, re-scanned and blended in as often as required.
The scan data are converted into firmware data formats (such as STL), usually exportable into third-party systems, using specific software and calculated to create a virtual, three-dimensional model which can be viewed on the monitor.
The data can be supplemented and further processed with additional CAD and CAM programmes e.g., for placing virtual implants, planning and fabricating restorations, abutments, drilling templates, bite raisers or producing real models. When used with manufacturing equipment (such as milling machines), restorations such as veneers, inlays, crowns or short-span bridgework can be fabricated in a single appointment.
Intraoral scanners are an increasingly relevant alternative to taking conventional impressions with elastomeric impression materials (PVS, polyether, etc.). Less material is required, breathing is not obstructed and gagging as well as risk of aspiration no longer occur. This very first important step already provides an entry-point to digital workflow, without having to “divert” via error-prone “real” impressions and models followed by scanning them with extraoral equipment (“lab scanners”).
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| lockjaw | Kiefersperre, Kieferklemme |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms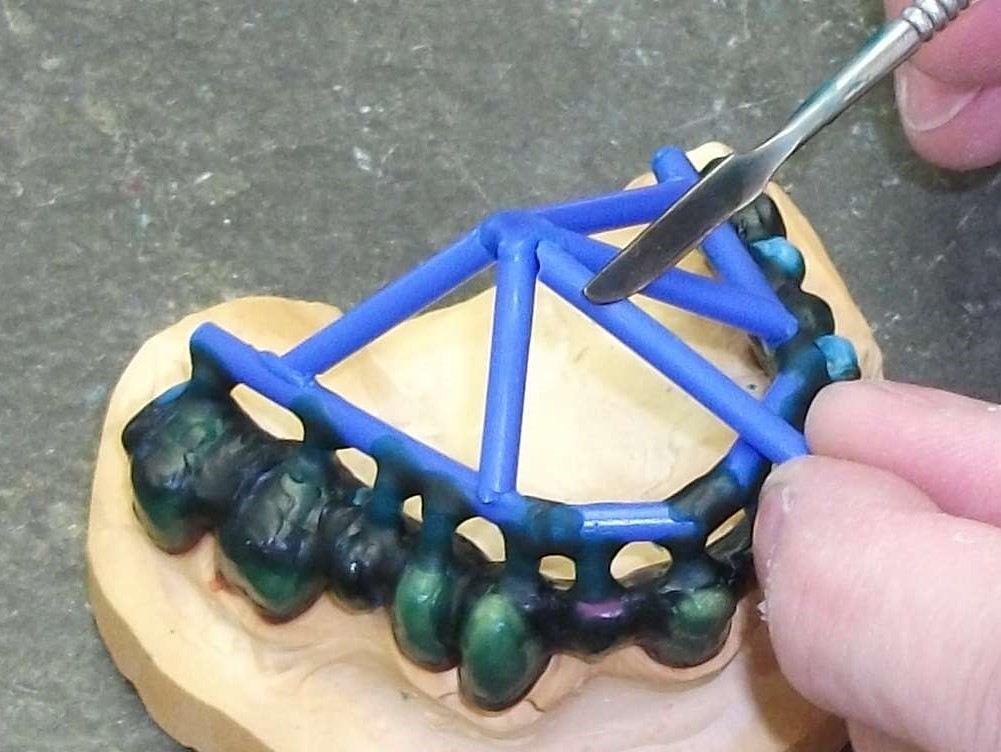 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument