Full dentures
Full dentures
Full dentures (also called complete dentures) are removable restorations. They replace all the teeth in an edentulous jaw, mainly using prefabricated acrylic denture teeth and less commonly made from porcelain. The denture base in the upper and lower jaw is generally made from acrylic (e.g. acrylates); in cases with particular requirements the hard palate of the upper jaw is covered by a metal palatal plate. There is no alternative restoration to full dentures without involving implants. An overdenture is a partial denture. An overdenture completely covers all elements connecting it to existing teeth or implants.
 Occlusal view of previous/new full dentures
Occlusal view of previous/new full dentures
As no information regarding occlusal height, occlusal relationship, tooth position etc. can be derived from existing teeth for full dentures, step-by-step reconstruction of intermaxillary relationship and soft-tissue support, function and aesthetics using anatomical conditions is a particular challenge. The consistency of measured values such as the mandibular rest position or the extent of its variability due to tooth loss and restoration is therefore debatable.
Diagnostic impressions of the jaw and, if applicable also an existing denture, are traditionally taken using stock trays for the fabrication of full dentures. Custom trays (functional trays) fabricated on the diagnostic models or existing dentures are used for taking functional impressions, after adaptation and additions (e.g. using thermoplastics, silicones). Positionally stable, slow-curing impression material (e.g. PVS) on the one hand produces different compression depending on the resilience of the mucosa, thus resulting in uniform pressure distribution to prevent pressure spots at a later stage. In addition, functional movements (swallowing, tongue, mouth, jaw and lip movements) are recorded to relieve anatomical and functional boundaries (e.g. mobile mucosal sections, fraenums or soft palate). The aim with full dentures in the upper jaw, therefore, is to achieve suction adhesion (distal post dam on the junction between the hard and soft palate, the palatal vibrating line); in the lower jaw the least objective is to have the denture rest in position.
 Full dentures viewed from the fitting surfaces
Full dentures viewed from the fitting surfaces
Bite registration and determination of the midline, occlusal plane and height are completed using templates with bite rims or arrow point tracing; these are checked, for example, using speech tests. Facebow transfer can be used for arbitrary hinge axis determination. A try-in of the prefabricated denture teeth set up in wax on the acrylic baseplate enables a check of the aesthetics, retention, occlusion, articulation and speech function prior to finishing. The denture is finished in the dental laboratory. Various procedures are used with cold and heat-curing acrylics, pressing, packing, syringing and pouring, flasks or overcasts etc. Following final adjustment of the occlusion and articulation, trimming and polishing the denture is fitted in the patient's mouth.
 Full dentures, lateral view
Full dentures, lateral view
In recent times this sequence with five to six appointments, which has been established for decades, has been considerably reduced (to two to three appointments) thanks to extensive digitisation. Different manufacturers offer the transfer of data acquired from the patient into a computer-supported virtual system. Digitised patient anatomy and prefabricated teeth or dental arches are placed in relationship to each other in a virtual articulator using CAD programmes and the denture base is then milled from a blank using a CAM process. The dental arches are either integrated in the milling blank pre-set (full denture is fabricated right away) or set up using prefabricated teeth (wax try-in and adjustment possible).
Fine adjustments after fitting can easily be made intraorally (spot grinding) and extraorally. A familiarisation and adaptation phase ranging from hours to weeks is to be expected. Any pressure spots that occur are relieved by grinding in the peripheries of the full denture. Incongruencies (spaces) between the denture and jaw caused by physiological or pressure-induced atrophy of the jaw (bone resorption) lead to deterioration of the retention and fit, rocking movements and food retention. This frequently results in worn denture teeth together with long-term bite closure. Functional integrity can be restored by relining the denture.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| piston release | Kolbenentriegelung |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms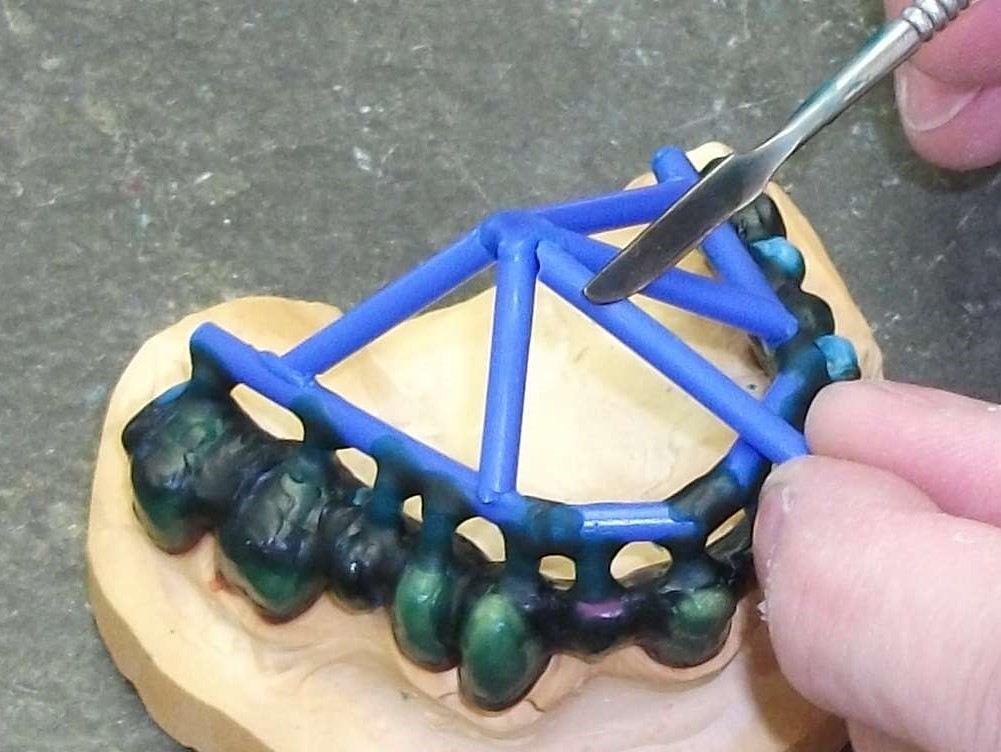 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument